The End of Daily Cholesterol Pills? “One-and-Done” Gene Edit Therapy That Stunned Cardiologists
You’ve likely been told that cholesterol control is a lifelong commitment. A daily statin. Regular blood tests. Constant vigilance. Miss a few doses, and your cardiovascular risk quietly rises again.
Here is the uncomfortable truth we see in Indian practice. Nearly 1 in 4 heart attacks occurs before the age of 50, often in patients already on treatment. Cholesterol control, as we practice it today, is necessary but not always sufficient.
This emerging gene therapy for cholesterol targets PCSK9 and may offer an alternative to lifelong statin use.
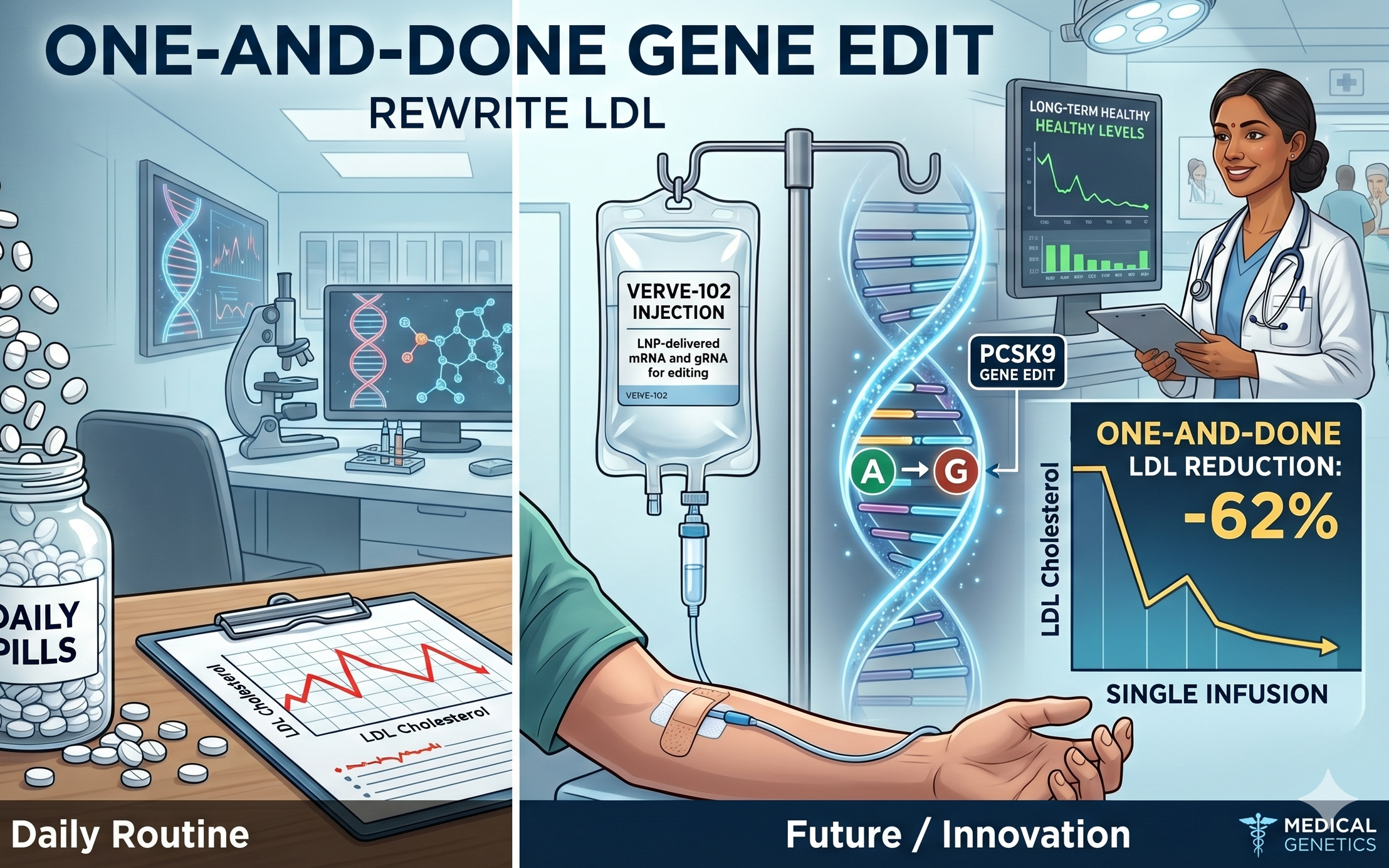
Now consider this shift. At the recent European Atherosclerosis Society Congress, a therapy called VERVE-102 showed that a single infusion reduced LDL cholesterol by up to 62 percent, with effects sustained beyond 18 months. Not daily suppression. A one-time genetic switch.
From Daily Statins to Genetic Precision: How We Got Here
For three decades, statins have been the foundation of prevention. They reduce cholesterol synthesis in the liver and lower LDL by 30 to 50 percent in most patients.
When that is not enough, we add:
- Ezetimibe: an additional 15 to 20 percent reduction
- PCSK9 monoclonal antibodies: up to 60 percent reduction, but require injections every 2 to 4 weeks
These therapies work. They have saved millions of lives. But they share one limitation. They require continuous use because the underlying biology remains unchanged.
VERVE-102 targets the control center itself.
In the Phase 1b Heart-2 trial involving 35 high-risk patients:
- PCSK9 protein fell by up to 88 percent
- LDL cholesterol dropped by up to 62 percent
- The effect persisted beyond 18 months, exceeding the normal liver cell lifespan
This durability suggests the genetic edit is maintained as new liver cells regenerate. That is the clinical significance of a one-time approach.
The Science That Changes the Equation: What Makes This Different
This therapy uses adenine base editing, a precise form of gene editing that changes a single DNA letter without cutting the DNA strand.
Mechanism, simplified:
- A lipid nanoparticle delivers mRNA instructions into liver cells
- The cell produces a base-editing enzyme
- A single nucleotide in the PCSK9 gene is altered
- The gene is permanently silenced
The delivery system is a critical upgrade. Earlier versions depended on LDL receptors for entry, which is unreliable in genetic cholesterol disorders.
VERVE-102 uses a GalNAc-conjugated nanoparticle, allowing entry via an alternate liver receptor pathway. This ensures consistent delivery even in severe cases.
Safety data from this early trial:
- No treatment-related serious adverse events
- No severe liver toxicity
- Mild, transient infusion-related symptoms only
What remains unproven is the outcome that matters most: whether this sustained LDL reduction will translate into fewer heart attacks and longer survival, as established with statins and PCSK9 inhibitors. That evidence will come only from long-term outcome trials now in progress.
A 15-year registry is already underway to track durability, off-target effects, and clinical endpoints.
Can Gene Therapy Replace Statins?
Gene editing therapies like VERVE-102 aim to permanently reduce LDL cholesterol by disabling the PCSK9 gene. While early results are promising, statins and PCSK9 inhibitors remain the standard of care until long-term outcome trials confirm safety and cardiovascular benefit.
Why This Matters More in Diabetes and Insulin Resistance
If you have diabetes, pre-diabetes, or central obesity, cholesterol behaves differently.
Insulin resistance alters LDL particles into:
- Small, dense LDL
- More prone to oxidation
- More likely to penetrate arterial walls
This is why many patients suffer heart attacks despite “acceptable” LDL levels.
Diabetic dyslipidemia is structurally more dangerous, not just numerically higher.
While gene editing is promising, it is not yet clinically available. What matters today:
- LDL targets below 55 mg/dL for high-risk patients
- Aggressive correction of insulin resistance
- Early identification of subclinical atherosclerosis
Waiting for future therapies while carrying high-risk lipid profiles is a preventable error.
The Pill Burden Problem: What Patients Actually Experience
A typical metabolic patient is managing:
- Diabetes or pre-diabetes
- Hypertension
- Dyslipidemia
This often means 4 to 6 medications daily.
Over time:
- Adherence drops
- Side effects accumulate
- Clinical control becomes inconsistent
The appeal of a one-time therapy is obvious. But until it becomes widely available, the real opportunity is precision simplification.
At a specialized metabolic clinic, the focus shifts to:
- Identifying root drivers such as insulin resistance and visceral fat
- Using advanced lipid markers like ApoB instead of relying only on LDL-C
- Reducing unnecessary medications while intensifying what actually works
The goal is not more prescriptions. It is fewer, smarter interventions with measurable outcomes.
What Should You Do Today? A Specialist’s Practical Guidance
Gene editing will likely enter clinical practice in phases over the next several years. Cost, access, and long-term safety data will determine its reach.
Your decisions today cannot wait for that timeline.
You should seek specialist evaluation now if you have:
- LDL cholesterol above 100 mg/dL with diabetes or pre-diabetes
- Triglycerides above 150 mg/dL
- A family history of heart attack before age 55 in men or 65 in women
- Evidence of fatty liver or abdominal obesity
- Previous cardiac event despite being on treatment
Immediate priorities:
1. Measure what matters
Go beyond standard lipid panels. Assess ApoB, triglyceride-to-HDL ratio, and inflammatory markers.
2. Correct insulin resistance at its root
This is the central driver of both diabetes and atherosclerosis.
3. Achieve risk-adjusted LDL targets
For high-risk individuals, this means below 55 mg/dL, not “within normal range.”
Summary Table
| Traditional UseModern DiscoveryPatient Benefit | ||
| Statins reduce LDL by 30–50% with daily dosing | Gene editing silences PCSK9 with a single intervention | Potential long-term LDL control |
| PCSK9 injections lower LDL by ~60% but require lifelong use | One-time infusion shows 62% LDL reduction sustained beyond 18 months | Reduced treatment burden |
| Focus on cholesterol levels alone | Targets genetic driver of cholesterol metabolism | Deeper, more durable risk reduction |
Take Control of Your Cardiovascular Risk Today
You do not need to wait for gene editing to protect your heart.
Advanced lipid optimization, cardiovascular risk screening, and targeted metabolic care are available today and can significantly reduce your risk when applied correctly.
If you have diabetes, pre-diabetes, or unexplained high cholesterol, the key question is not whether your report is “normal.” It is whether it is safe for your metabolic profile.
Speak to our specialists to design a precise, evidence-based prevention plan tailored to you.
Contact our Mumbai clinics to book an assessment:
- Worli Clinic: +91 79778 20388
- Andheri Clinic: +91 89280 41793
- Goregaon Clinic: +91 83690 71795
Medical Disclaimer
This content is for educational purposes only and is not a substitute for professional medical advice. Individuals with existing medical conditions or high cardiovascular risk should consult their healthcare provider before making changes to their treatment plan.
Article Author
Dr Kamales Kumar Saha
Clinician–Leader · Cardiac Surgeon · Preventive Cardiologist · IICA-Certified Independent Director
Author: The Silent Epidemic
Dr Kamales Kumar Saha combines over three decades of surgical expertise with a focused mission on preventing premature cardiovascular disease through targeted metabolic care.
Copyright Notice
© 2026 Dr Kamales Kumar Saha. All rights reserved.
No part of this blog may be reproduced, stored, or transmitted in any form without prior written permission of the author, except for brief quotations used in reviews or scholarly references.



